The use of SilverPlug® within a state-of-the-art implant placement case.
Dr. Minas Leventis, DDS, MSc, PhD.
A 70-year-old female patient, non-smoker, with non-contributory medical history presented with a failing upper right central incisor (UR1) due to non-restorable subgingival cervical caries. The treatment plan consisted of extraction of UR1, immediate implant placement with immediate loading with a temporary crown, and placement of the final restoration 4 months later.
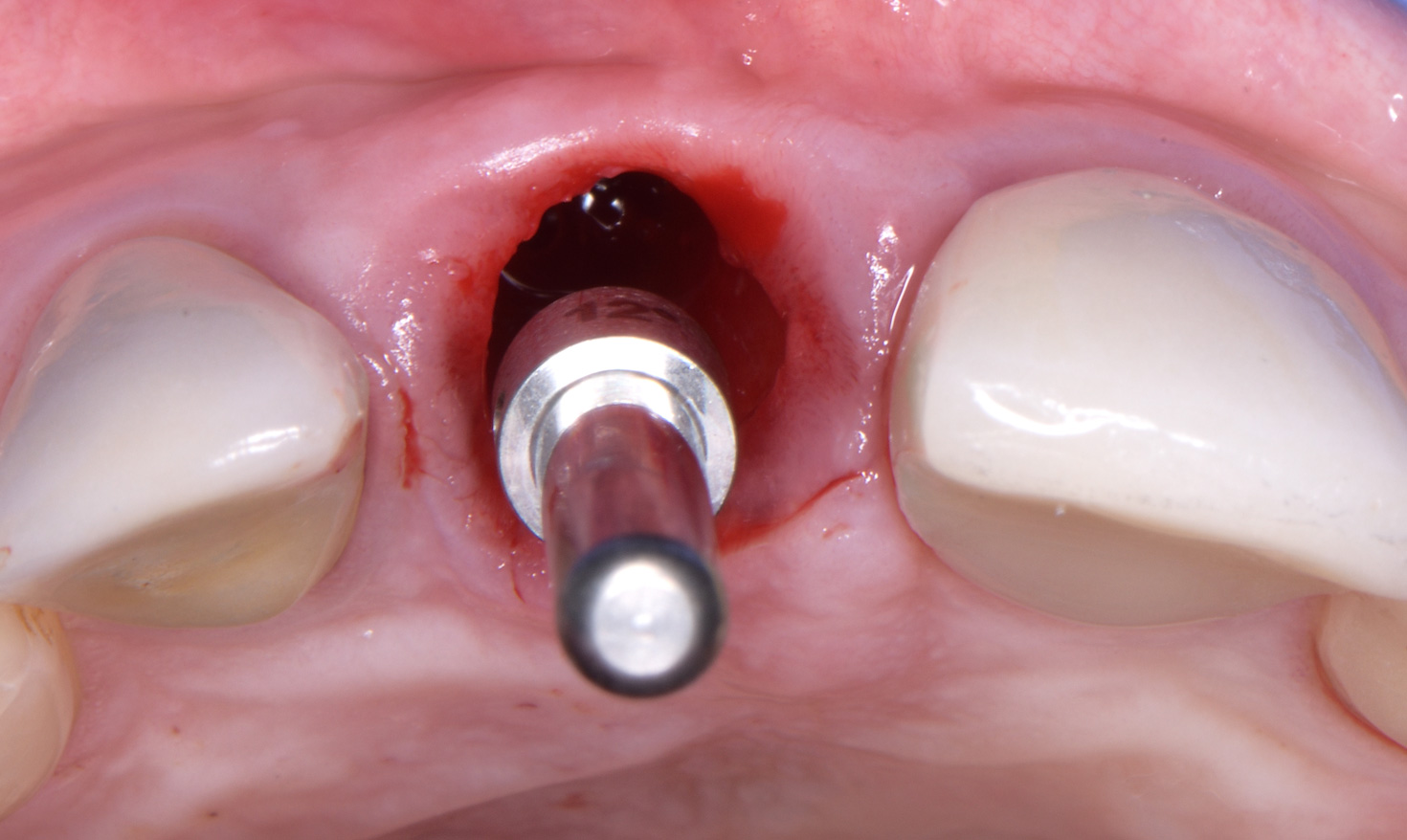
The “atraumatic” flapless removal of UR1 is important in order not to damage the surrounding hard tissues and to preserve intact the supra-crestal gingival complex.
After thorough debridement of the socket with Lucas curettes, a sharp pilot drill was used to create the initial osteotomy. A co-axis 12° direction guide pin was used to verify the correct direction of the initial osteotomy, as an implant with a 12° angle correction of the implant-abutment interface will be placed.
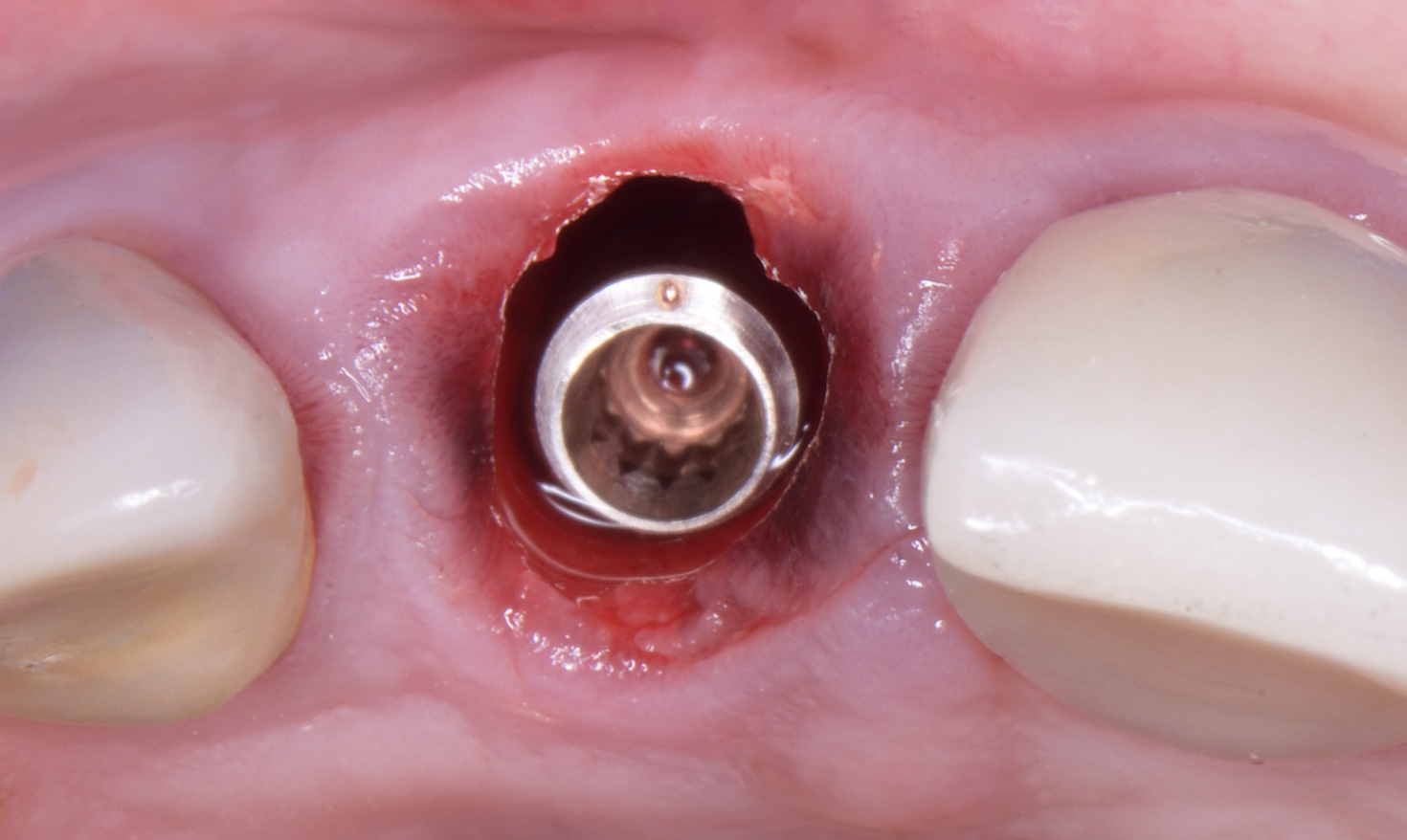
The osteotomy was finalized using the specific drill shank and a Southern Inverta body-shift 12° co-axis implant was placed, achieving excellent initial stability. Both bone and soft tissue zones were grafted using a synthetic b-TCP/Calcium Sulfate bone substitute. A prefabricated PEEK temporary cylinder was connected and a screw-retained temporary crown was fabricated.
The access hole of the provisional crown was sealed with SilverPlug®.
Oxygen-releasing Bluem oral gel was applied immediately post-op and given to the patient to use at home twice a day for a week. Amoxicillin 500mg x 3 for 5 days and paracetamol were prescribed.
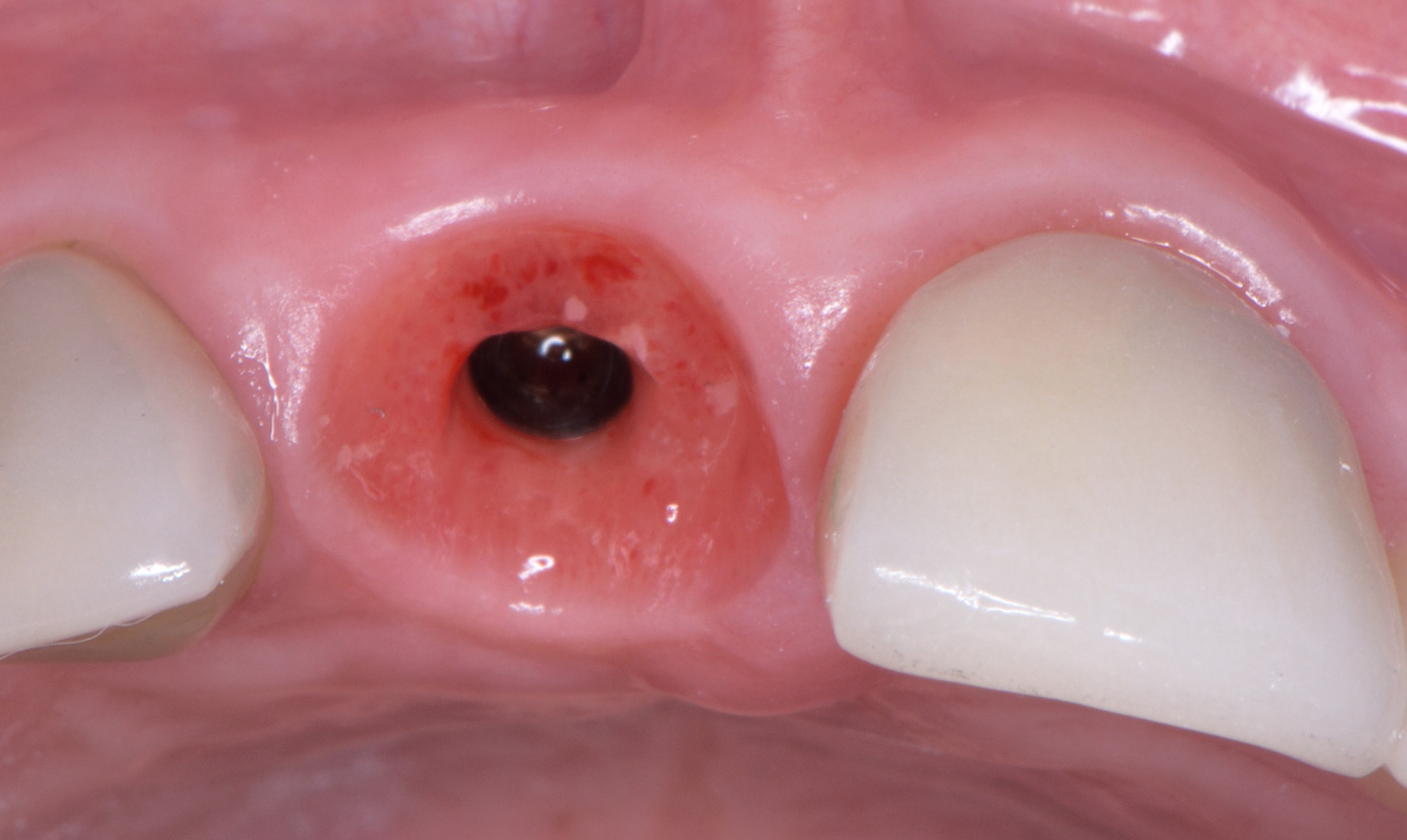
The clinical view 4 months post-op shows very healthy keratinized soft tissues and excellent preservation of the architecture of the ridge. No inflammation, no smell when removing the temporary crown.
Final screw-retained restoration. Zirconia crown on a custom base Atlantis anodized abutment. Scrubbing with oxygen-releasing Bluem solution to disinfect the prosthetic canal, and sealing with SilverPlug@.
2.5 months after loading the final restoration, the soft tissues mature and the papillae grow back. The design and 3D positioning of the implant, the emergence profile of the provisional and final restorations, the absence of soft tissue inflammation and the quality of the regenerated bone are among the important factors which affect our results.
Dr. Leventis holds a PhD (2010) and an MSc (2004) in Oral Surgery from the Dental School of University of Athens, Greece. In 2008 he also attended a post-graduate program in Periodontics and Implantology at the University of Heidelberg, Germany.
From 2002 to 2014 he was a Clinical Fellow at the University Department of Oral & Maxillofacial Surgery, Children’s Hospital of Athens “P. & A. Kyriakou”, Athens, Greece.
Dr. Leventis is currently on the Faculty of the Dental School, University of Athens as a Visiting Clinical Instructor and Researcher, where he teaches under and post-graduate students Exodontia, Oral Surgery, Bone Grafting and Implantology, while undertaking extensive experimental research.
Dr. Leventis has been invited to lecture extensively throughout the world on a variety of scientific topics in Oral Surgery. He is the author of numerous scientific articles published in international peer reviewed journals like Journal of Cranio-Maxillofacial Surgery, TripleO, Implant Dentistry, Clinical Oral Investigations, Compendium and EDI Journal.
Based downtown London his private work and clinical research are focused on Oral Surgery, Tissue Engineering and Implant Dentistry. He is a member of many prestigious International and British scientific societies, in 2012 he earned the Diplomate status of the International Congress of Oral Implantologists (ICOI), is an active member of ADI (UK), a member of Leading Implant Centers and a founding member of ICOI-Hellas (Greece).